
Introduction
The Mini-Mental State Examination (MMSE) is a widely-used,
brief cognitive screening tool designed to evaluate the cognitive state of
individuals, particularly those suspected of having Alzheimer's disease or
other forms of dementia. Developed by Folstein and colleagues in 1975, the MMSE
assesses various cognitive domains, including orientation, registration,
attention, calculation, recall, language, and visual-spatial skills. This
article aims to provide a comprehensive guide on the MMSE for Alzheimer's assessment,
including its administration, scoring, and interpretation of results.

MMSE Administration
The MMSE is a structured, paper-and-pencil test that can be
administered by healthcare professionals, such as physicians, nurses, and
psychologists, in approximately 5-10 minutes. The test consists of 30
questions, each scored on a 0 - 1 or 0 - 2 point scale, with a maximum total
score of 30 points. The questions are divided into the following categories:
- Orientation:
Five questions assess the individual's awareness of time and place (e.g.,
"What is the year?", "Where are we right now?").
- Registration:
Three questions assess the individual's immediate recall of three
unrelated words (e.g., "Repeat these words after me: apple, table,
pen.").
- Attention
and Calculation: Five questions assess the individual's ability to
concentrate and perform simple arithmetic (e.g., "Spell 'world'
backwards, and then repeat the three words from before.").
- Recall:
One question assesses the individual's ability to remember the three
previously presented words (e.g., "What were the three words I asked
you to remember earlier?").
- Language:
Eight questions assess the individual's ability to understand and produce
language, including naming objects, repeating phrases, following commands,
reading, and writing (e.g., "Show me two fingers.").
- Visual-Spatial
Skills: One question assesses the individual's ability to copy a simple
design (e.g., "Please draw this shape for me.").
Details
1.
Orientation (10 points):
·
Ask for the date. Then specifically ask for
parts omitted (e.g., "Can you also tell me what season it is?"). One
point for each correct answer.
·
Ask in turn, "Can you tell me the name of
this hospital (town, county, etc.)?" One point for each correct answer.
2.
Registration (3 points):
·
Say the names of three unrelated objects clearly
and slowly, allowing approximately one second for each. After you have said all
three, ask the patient to repeat them. The number of objects the patient names
correctly upon the first repetition determines the score (0-3). If the patient
does not repeat all three objects the first time, continue saying the names
until the patient is able to repeat all three items, up to six trials. Record
the number of trials it takes for the patient to learn the words. If the
patient does not eventually learn all three, recall cannot be meaningfully
tested.
·
After completing this task, tell the patient,
"Try to remember the words, as I will ask for them in a little
while."
3.
Attention and Calculation (5 points):
·
Ask the patient to begin with 100 and count backward
by sevens. Stop after five subtractions (93, 86, 79, 72, 65). Score the total
number of correct answers.
·
If the patient cannot or will not perform the
subtraction task, ask the patient to spell the word "world" backwards.
The score is the number of letters in correct order (e.g., dlrow=5, dlorw=3).
4.
Recall (3 points):
·
Ask the patient if he or she can recall the
three words you previously asked him or her to remember. Score the total number
of correct answers (0-3).
5.
Language and Praxis (9 points):
·
Naming: Show the patient a wrist watch and ask
the patient what it is. Repeat with a pencil. Score one point for each correct
naming (0-2).
·
Repetition: Ask the patient to repeat the
sentence after you ("No ifs, ands, or buts."). Allow only one trial.
Score 0 or 1.
·
3-Stage Command: Give the patient a piece of
blank paper and say, "Take this paper in your right hand, fold it in half,
and put it on the floor." Score one point for each part of the command
correctly executed.
·
Reading: On a blank piece of paper print the
sentence, "Close your eyes," in letters large enough for the patient
to see clearly. Ask the patient to read the sentence and do what it says. Score
one point only if the patient actually closes his or her eyes. This is not a
test of memory, so you may prompt the patient to "do what it says"
after the patient reads the sentence.
·
Writing: Give the patient a blank piece of paper
and ask him or her to write a sentence for you. Do not dictate a sentence; it
should be written spontaneously. The sentence must contain a subject and a verb
and make sense. Correct grammar and punctuation are not necessary.
6.
Copying:
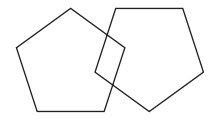
·
Show the patient the picture of two intersecting
pentagons and ask the patient to copy the figure exactly as it is. All ten
angles must be present and two must intersect to score one point. Ignore tremor
and rotation
Scoring and Interpretation of Results
The MMSE is scored by adding up the points obtained from
each question, with a maximum total score of 30 points. A higher score
indicates better cognitive function. The following guidelines can be used to
interpret the results:
- A
score of 24-30 points suggests normal cognitive function.
- A
score of 19-23 points indicates mild cognitive impairment, which may be
indicative of early-stage Alzheimer's or other forms of dementia.
- A
score of 10-18 points indicates moderate cognitive impairment, which is
often associated with moderate Alzheimer's disease.
- A
score of 9 points or less indicates severe cognitive impairment, which is
characteristic of advanced Alzheimer's disease.
It is essential to note that the MMSE is not a diagnostic
tool for Alzheimer's disease but rather a screening test that can help identify
individuals who may require further evaluation by a specialist. The test's
sensitivity and specificity vary depending on the population being tested, and
additional diagnostic tests, such as neuropsychological assessments, brain
imaging, and laboratory tests, are often required to confirm a diagnosis of
Alzheimer's disease.
Benefits
·
Quick screening tool
MMSE is designed to be a quick screening tool for
cognitive impairment. This is why it's a widely used resource for healthcare
professionals: its simplicity makes it easy to screen patients.
·
Standardization
MMSE provides a standardized set of questions, scoring
methods, and interpretation for healthcare professionals.
·
Early diagnosis
Mini-Mental State Examinations can give you a glimpse of
a patient's cognitive function. If the score is low, you can use that as a
starting point for further evaluation and early intervention.
Limitations of the MMSE
While the MMSE is a valuable tool for cognitive screening,
it has several limitations that should be considered when interpreting the
results:
- Educational
and cultural factors: The MMSE may underestimate the cognitive abilities
of individuals with lower educational levels or those from different
cultural backgrounds.
- Language
barriers: The test relies heavily on language skills, which may be
challenging for non-native English speakers or those with language
impairments.
- Sensitivity
to depression: The MMSE may be influenced by the presence of depression,
which can affect cognitive function.
- Ceiling
and floor effects: The MMSE may not be sensitive enough to detect subtle
cognitive changes in individuals with high baseline cognitive function
(ceiling effect) or severe cognitive impairment (floor effect).
Conclusion
The Mini-Mental State Examination (MMSE) is a widely-used
cognitive screening tool that can help identify individuals who may require
further evaluation for Alzheimer's disease or other forms of dementia. By
assessing various cognitive domains, the MMSE provides valuable information on
an individual's cognitive function and can guide healthcare professionals in
determining the need for additional diagnostic tests and interventions.
However, it is essential to recognize the limitations of the MMSE and interpret
the results in the context of the individual's educational, cultural, and
linguistic background.
